News & Announcements
Resolving Inflammation in COVID-19
Article from 2020-06-11
Calming the eicosanoid storm to quell the cytokine storm
Not all patients with COVID-19 develop the same symptoms, but the hallmarks of a severe SARS-CoV-2 infection include an excessive immune response with a disproportionate release of cytokines and extreme inflammation. This can lead to acute respiratory distress syndrome (ARDS) and pneumonia, culminate in cardiac, lung, and renal system failure, and ultimately cause death. This dysregulated cytokine release is better known as the cytokine storm. A related inflammatory response driven by pro-inflammatory eicosanoids is also triggered and has been called the eicosanoid storm.
Cytokine Storm
In patients with COVID-19, the cytokine storm involves elevated levels of pro-inflammatory and anti-inflammatory cytokines or chemokines, including TNF-α, IFN-γ, IL-1 receptor antagonist (IL-1RA), IL-2RA, IL-6, IL-10, IL-18, hepatocyte growth factor (HGF), monocyte chemotactic protein-3 (MCP-3/CCL7), monokine induced by IFN-γ (MIG), macrophage colony-stimulating factor (M-CSF), granulocyte colony-stimulating factor (G-CSF), MIG-1α, cutaneous T cell-attracting chemokine (CTACK), and IFN-γ-induced protein 10 (IP-10/CXCL10). Levels of IP-10, MCP-3, and IL-1RA are significantly higher in severe cases and are associated with increased viral load, loss of lung function, lung injury, and a fatal outcome.1 Assays can be performed to determine elevated cytokine levels.
To help keep inflammation under control, T regulatory cells (Tregs) are recruited to the storm where they can neutralize inflammatory cytokine secretion by inhibiting neutrophil extravasation via IL-10, promote apoptosis of neutrophils, and encourage phagocytosis of dead neutrophils by macrophages. Tregs also inhibit monocyte activity and survival as well as stimulate macrophage polarization toward an anti-inflammatory phenotype through the release of anti-inflammatory cytokines. Thus, any increases of IL-10 in severe COVID-19 might represent a feedback loop attempting to counteract systemic and local inflammation.
An increased neutrophil-to-lymphocyte ratio in the blood is also an indicator of a cytokine storm, and lymphopenia is seen in severe cases of COVID-19. Indeed, serum levels of TNF-α, IL-6, and IL-10 inversely correlate with a reduction in T cell numbers.2 The associated rise in these cytokines likely drives the depletion and exhaustion of T cell populations. Depletion of tissue-resident alveolar macrophages and the accumulation of monocyte-derived inflammatory macrophages is also associated with disease severity.3 Inflammatory macrophages enact programs to produce cytokines implicated in the cytokine storm. Thus, therapeutic strategies using cytokine-specific inhibitors that target myeloid cells in the lung immune microenvironment are being examined to treat COVID-19-associated inflammation. For example, the anti-human IL-6 receptor monoclonal antibody tocilizumab, approved for treatment of rheumatoid arthritis, is undergoing clinical trials to establish its effectiveness in alleviating COVID-19 pneumonia.4 The monoclonal antibody-based therapy works by blocking cellular IL-6 receptors. Several established immunosuppressive agents, such as broadly acting anti-inflammatory corticosteroids, can also effectively overpower cytokine storms. For example, dexamethasone, the synthetic glucocorticoid, has been shown to reduce deaths by a third in patients hospitalized with Covid-19 in the RECOVERY (Randomised Evaluation of COVid-19 thERapY) trial. Its complex effects act primarily through inhibition of inflammatory cells and suppression of expression of inflammatory mediators.
Controlling this inflammatory response is critically important for patient survival and preventing pathological fibrosis. But suppressing the immune system while fighting viral infection should be considered heavily since this can enable the virus to continue replicating and weaken the ability to fight off any secondary infection. For this reason, cytokine inhibitor therapies are best employed along with an antiviral agent. Another concern with specific IL-6 inhibition is that it blocks the action of only one cytokine late in the inflammation process. By combining inhibitors to block more than one component of the cytokine storm, this issue may be addressed. However, inflammation may be blocked with this approach without enabling the initiation of resolution and repair systems.
Eicosanoid Storm
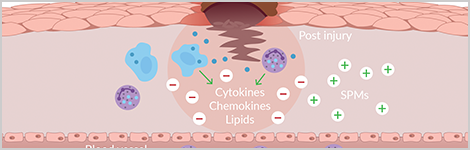
The cytokine storm is not an isolated event but occurs in a larger context where inflammasomes are activated by the colossal cell death occurring in its wake. The cellular debris triggers a surge of pro-inflammatory bioactive lipid mediators, including prostaglandins and leukotrienes, that drive a local inflammatory response.5 This inflammation is thought to be cleared by an active biochemical process that stimulates macrophage phagocytosis and efferocytosis and counters pro-inflammatory cytokine production through specialized pro-resolving lipid mediators (SPMs), such as resolvins.6 SPMs derived from ω-3 fatty acids, primarily eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), promote a return to tissue homeostasis. However, a deficit in this resolution process could lead to hyper-inflammation.
SPMs demonstrate antiviral activity against influenza without being immunosuppressive and can promote antiviral B cell antibody production and lymphocyte activity, indicating they may have usefulness in treating SARS-CoV-2 infection. Indeed, Recchiuti et al. have shown that resolvin D1 and resolvin D2 reduce SARS-CoV-2-induced cytokine and chemokine release in macrophages.717-hydroxy Docosahexaenoic acid (17-HDHA) and additional SPM precursors have shown promise as adjuvants in primary influenza vaccines.8
Epoxyeicosatrienoic acids (EETs) can also stimulate inflammation resolution by promoting the production of pro-resolution mediators, such as lipoxins, and activating anti-inflammatory processes. EETs are rapidly metabolized by soluble epoxide hydrolase (sEH), but their levels can be stabilized with the use of sEH inhibitors.
Both resolvins and EETs are known to diminish thrombosis, a complication associated with COVID-19 progression. Compared to conventional anti-inflammatory agents, such as NSAIDs and cyclooxygenase-2 inhibitors that indiscriminately inhibit eicosanoid pathways thereby thwarting the production of resolution mediators, SPMs and sEH inhibitors are more targeted in their ability to promote endogenous inflammation resolution mechanisms and enable a return to tissue homeostasis. Thus, Panigrahy and colleagues suggest that those SPMs and sEH inhibitors that are currently in clinical trials for other inflammatory diseases should be examined in the context of COVID-19 to control the local and systemic inflammatory response.6 Rather than just blocking individual cytokines, moving upstream to modulate them by stimulating their clearance and promoting cellular repair is the body's natural way to turn off inflammation. Soluble epoxide hydrolase (sEH) inhibitors and resolvins may be as important as the antiviral therapies being explored to alleviate symptoms of the disease. Drs. Dipak Panigrahy and Bruce Hammock tell us that EC5026, the EicOsis oral drug candidate for neuropathic pain with FDA fast-track designation, and EC1153, a more water-soluble, short-lived version that finished Phase IIA clinical trials in humans with no adverse events, may be suitable drug candidates to treat patients with COVID-19.9 They propose that these drugs will alleviate the cytokine storms that occur when the immune system is overwhelmed as the patient is battling for survival.
Key Tools for Tracking Cytokine and Eicosanoid Storms
Cayman offers single-plex and multi-plex ELISA kits to study the cytokine storm and has synthesized an array of key lipid mediators as biochemical tools or standards for mass spectrometry and developed ELISAs to aid in understanding the role of SPMs in resolving the eicosanoid storm. sEH inhibitors are also available to modulate the concentration of EETs and other fatty acid epoxides.
You May Also Be Interested In
 SPM Research Tools |  Download a Free SPM Lab Wall Poster | |
|---|---|---|


References
1. Yang, Y., Shen, C., Li, J., et al. Exuberant elevation of IP-10, MCP-3 and IL-1ra during SARS-CoV-2 infection is associated with disease severity and fatal outcome. medRxiv (2020).
2. Diao, B., Wang, C., Tan, Y., et al. Reduction and functional exhaustion of T cells in patients with coronavirus disease 2019 (COVID-19). medRxiv (2020).
3. Liao, M., Liu, Y., Yuan, J., et al. The landscape of lung bronchoalveolar immune cells in COVID-19 revealed by single-cell RNA sequencing. medRxiv (2020).
4. Xu, X., Han, M., Li, T., et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA117(20), 10970-10975 (2020).
5. Dennis, E.A. and Norris P.C. Eicosanoid storm in infection and inflammation. Nat. Rev. Immunol.15(8), 511-523 (2015).
6. Panigrahy, D., Gilligan, M.M., Huang, S., et al. Inflammation resolution: A dual-pronged approach to averting cytokine storms in COVID-19? Cancer Metastasis Rev. (2020).
7. Recchiuti, A., Patruno, S., Mattoscio, D., et al. Resolvin D1 and D2 reduce SARS-CoV-2-induced inflammatory responses in cystic fibrosis macrophages. FASEB J.35(4), e21441 (2021).
8. Ramon, S., Baker, S.F., Sahler, J.M., et al. The specialized proresolving mediator 17-HDHA enhances the antibody-mediated immune response against influenza virus: A new class of adjuvant? J. Immunol. 193(12), 6031-6040 (2014).
9. Personal conversation with Dipak Panigrahy and Bruce Hammock.
Contact Info
Cayman Chemical1180 East Ellsworth RoadAnn Arbor, Michigan 48108 USAToll Free: (800) 364-9897(USA and Canada only)Fax: (734) 971-3640